
One Simple Trick to Save Medicare $1 Billion
/An article appearing in the Journal of the American Medical Association finds we are paying through the nose for combination pills.
Would you like to save about a billion dollars?
This article, appearing in the Journal of the American Medical Association may have the solution.

Many of the studies I discuss are complex, with advanced statistical concepts, and lots of subtleties of interpretation. This one? Well, it can basically be summed up as follows:

This is Exforge, a pill containing both the angiotensin receptor blocker valsartan and the calcium-channel blocker amlodipine. It costs $8.21 per pill.
This is two pills, the angiotensin-receptor blocker valsartan and the calcium channel blocker amlodipine. Together, they cost $0.96.
You get it right? The combo drug is way, way more expensive.
And that’s largely because, as current law stands, pharmaceutical companies can extend some market exclusivity of a drug that is nearly about to come off-patent by mixing it with some other drug.
The authors of the JAMA paper asked a simple question. How much money could we save if Medicare bought the constituent pills instead of the combo pill?
The answer? About a billion dollars.
The authors used data published by Medicare which identifies the number of individuals taking various drugs and the price.
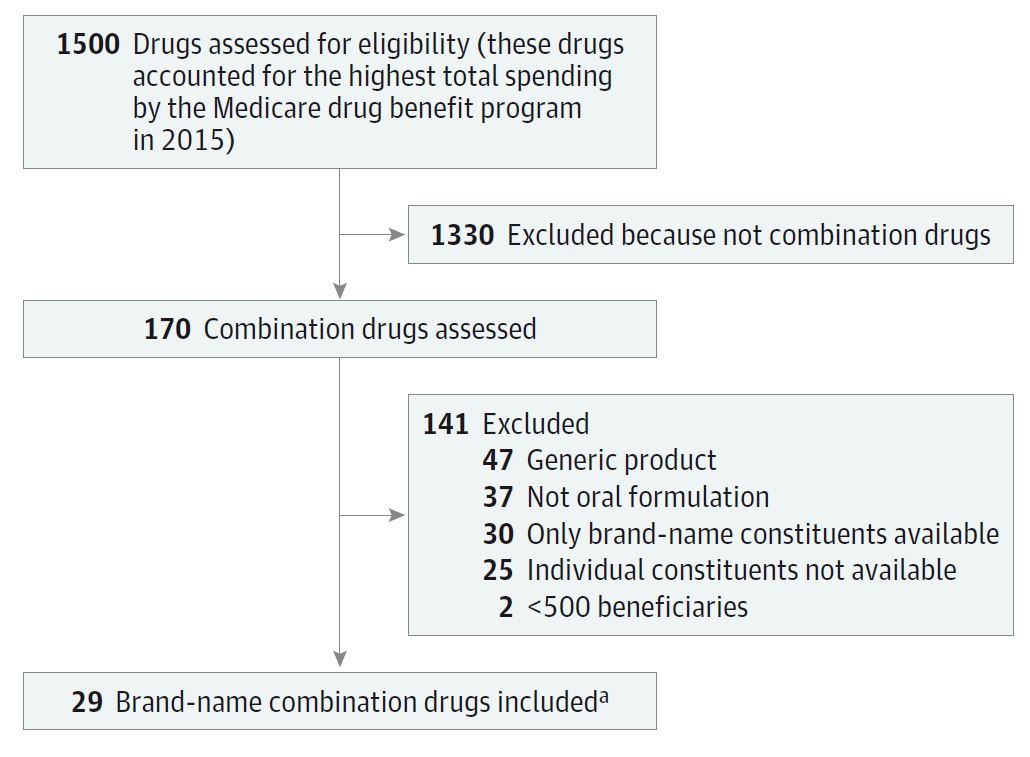
Flow diagram demonstrating how they found the 29 eligible combo pills from the 1500 drugs we spend the most money on.
They focused on the 1500 drugs that accounted for the most spending in the Medicare program. Of those, 170 were combo drugs. But most were either already generic, or one of the components didn’t have a generic equivalent. In fact, there were only 29 brand-name combo drugs that you could conceivably break down into its generic parts.
You know a lot of these names – I have prescribed some of them: Diovan-HCT, Percocet, Fosamax plus D. And I suppose, in the back of my head, I know the combo pills are more expensive, but I really didn’t appreciate just how much more expensive they are.
If I prescribe oxycodone and acetaminophen, CMS pays $0.38 per dose. If I prescribe Percocet, CMS pays $14.23 per dose – a 37-fold increase. You may of course ask why Medicare agrees to such exorbitant prices for these combo pills but that, my friends, is a topic for another time.
We’re not talking about a lot of drugs here, but we are talking about a lot of money. If we split up all of these 29 combo pills, we’d save Medicare 925 million dollars.
Now, some of you may be thinking that one pill is way more convenient than two or three, and maybe that would even increase adherence which might improve outcomes. There’s not much data supporting that idea, actually, as this Cochrane review shows:

But look at it on the patient level.
If we took all our patients on Diovan-HCT and switched them to Valsartan and Hydrochlorothiazide, we could give them each $1750 dollars a year in cash and still come out even. That might be worth a bit of inconvenience, right?
How does this problem get fixed? Three solutions. First, Medicare can put its foot down and stop paying for combination pills. Second, the FDA can stop granting market exclusivity for combination pills when the constituents are not novel agents.
I’m not sure why these changes haven’t happened, but this figure might have something to do with it.

So, as ever, it’s up to us, those with the power of the prescription pad to peddle pills more perspicaciously.
This post first appeared on medscape.com.