
Overburdened: The High Suicide Rate of Healthcare Workers
/Health aides — like nursing assistants and home health aides at particular risk.
If you run into a healthcare provider these days and say “how are you doing?” you’re likely to get a response like – “you know, hanging in there”. And you smile and move on. But it may be time to go a step farther. If you ask that next question – “no, really, how are you doing?” Well – you might need to carve out some time.
It’s been a rough few years for those of us in the healthcare professions. Our lives, dominated by COVID-related concerns at home, were equally dominated by COVID-concerns at work. On the job, there were fewer and fewer of us around as exploitation and COVID-related stressors led doctors, nurses, and others to leave the profession entirely or take early retirement. Even now, I’m not sure we’ve recovered. Staffing in the hospitals is still a huge problem – and the persistence of impersonal meetings via teleconference, which not only prevent any sort of human connection but – audaciously – run from one to the other without a break – robs us of even the subtle joy of walking from one hallway to another for five minutes of reflection before sitting down to view the next hastily-cobbled together PowerPoint.
Speaking in generalities of course.
I’m talking about how bad things are now because, in truth, they’ve never been great – and that may be why healthcare workers – people with jobs focused on serving others – are nevertheless at substantially increased risk of suicide.
Analyses through the years have shown that physicians tend to have higher rates of death from suicide than the general population. There are reasons for this that may not entirely be due to work-related stress – doctor’s suicide attempts are more often lethal – we know what is likely to work, after all.
But a focus on physicians fails to acknowledge the much larger population of people who work in healthcare, are less well-compensated, have less autonomy, and do not hold as respected a position in society. And, according to this paper in JAMA, it is those people who may be suffering most of all.

The study is a nationally-representative sample based on the 2008 American Community survey. Records were linked to the National Death Index through 2019.
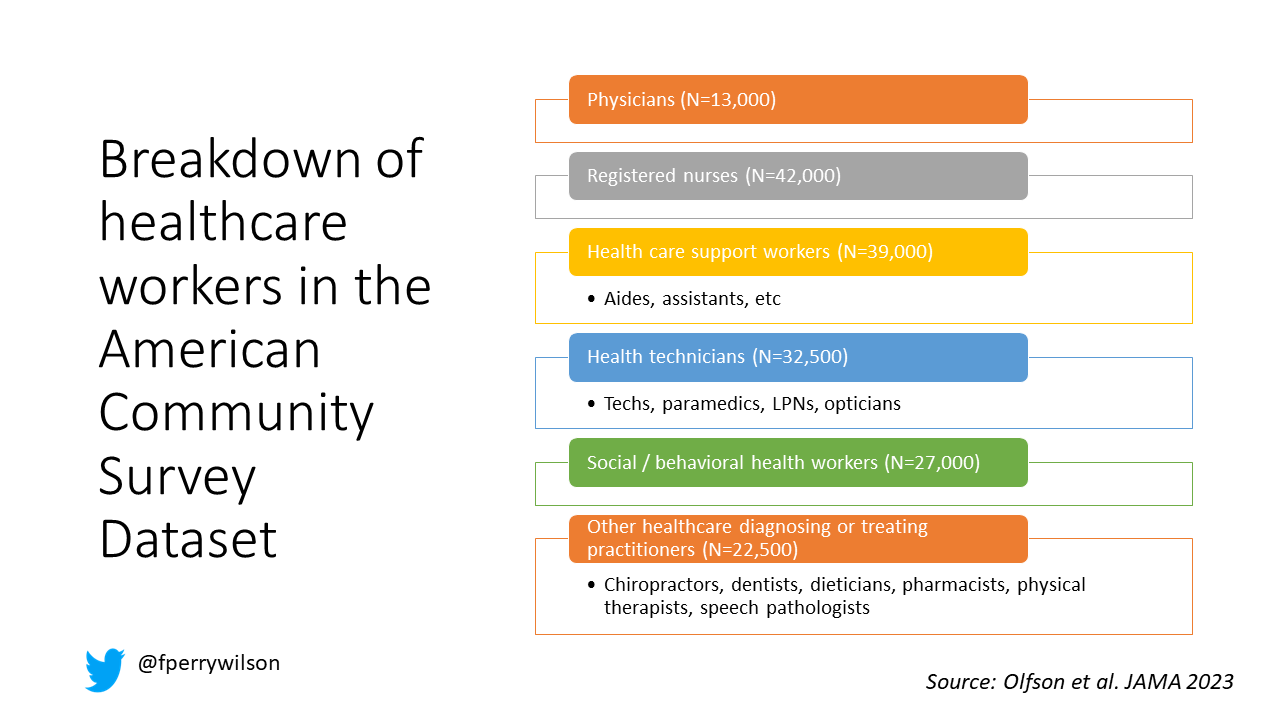
Survey respondents were classified into five categories of health care worker, as you can see here. 1,666,000 non-healthcare workers served as the control group.
Let’s take a look at the numbers.
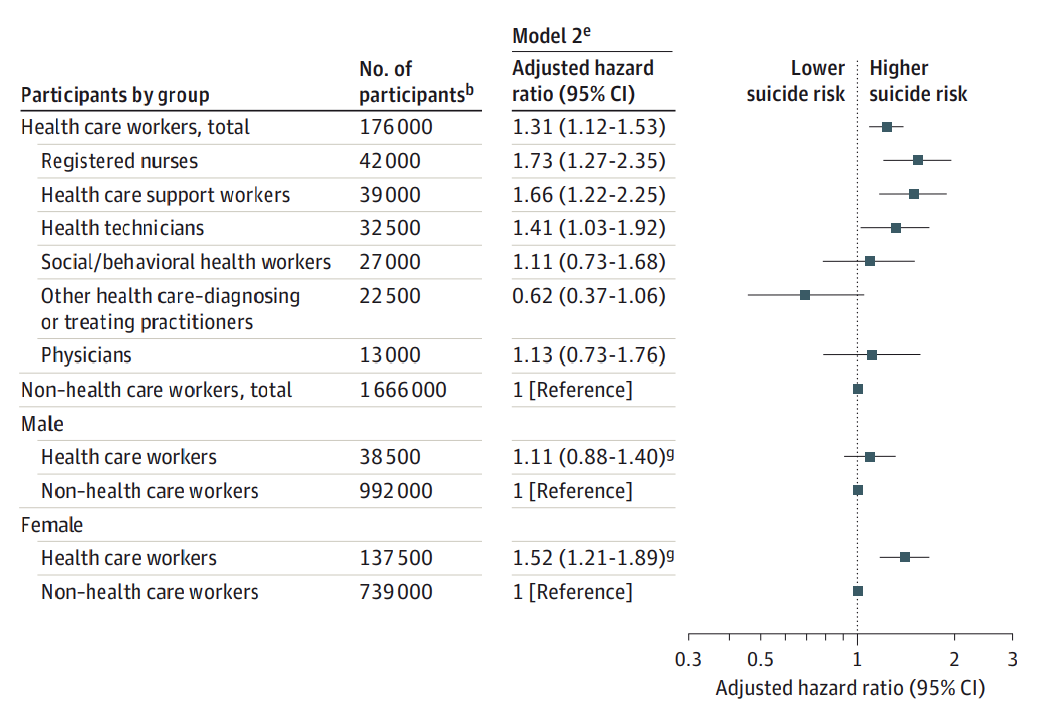
I’m showing you age and sex-standardized rates of death from suicide starting with non-healthcare workers. In this study, physicians have similar rates of death from suicide to the general population. Nurses have higher rates, but health care support workers – nurses aides, home health aides, have rates nearly twice that of the general population.

Only social and behavioral health workers had rates lower than the general population – perhaps because they know how to access life-saving resources.
Of course, these groups differ in a lot of ways – education and income for example. But even after adjustment for these factors as well as sex, race, and marital status, the results persist. The only group with even a trend towards lower suicide rates are social and behavioral health workers.
There has been much hand-wringing about rates of physician suicide in the past. It is still a very real problem. But this paper, finally, highlights that there is a lot more to the healthcare profession than physicians. It’s time we acknowledge and support the people in our profession who seem to be suffering more than any of us – the aides, the techs, the support staff – the overworked and underpaid who have to deal with all the stresses physicians like me face and then some.
There’s more to suicide risk than just your job – I know that. Family matters. Relationships matter. Medical and psychiatric illnesses matter. But to ignore this problem when it is right here, in our own house so to speak, can’t continue.
Might I suggest we start by asking someone in our profession – whether doctor, nurse, aide, or tech, how they are doing. How they are really doing. And when we are done listening – we use what we hear to advocate for real change.
A version of this commentary first appeared on Medscape.com.